

The beginning:
Without anyone yet realizing it, history was made on Tuesday, June 13, 1978. The treatment of heart attacks (“acute myocardial infarctions”) would be changed forever with the first ever primary percutaneous coronary intervention (PCI), the procedure we use today to restore blood flow to the heart. Early that afternoon, Dr. Peter Rentrop received an emergency call from the Cardiac Catheterization Lab at the University Medical Center in Göttingen, Germany, which he headed at the time. There was a serious complication. The catheterization team was assembled around a patient complaining of severe chest pain. The electrocardiogram displayed on the monitor indicated an acute heart attack involving the back part of the heart (the ”inferior wall”). The patient, a 45-year-old truck driver, with a history of heavy smoking and high blood pressure, had been hospitalized nine months earlier for a heart attack also to the inferior wall. After discharge in October 1997, he still had burning in his chest when walking up hill or climbing stairs. One month before his current admission this discomfort had become more frequent, even at complete rest. Because of his worsening symptoms he now underwent coronary angiography.
What is coronary angiography?
Coronary angiography is an invasive procedure which visualizes the channel of the blood vessels feeding the heart muscle, the coronary arteries and reveals blockages in these vessels. Contrast material is injected into the coronary arteries through a thin plastic tube, called a catheter, which is advanced from an artery either in the leg or an arm to the origin of the coronary arteries. Flow of the contrast material through the coronary arteries is visualized and filmed using X-rays.
History in the making:
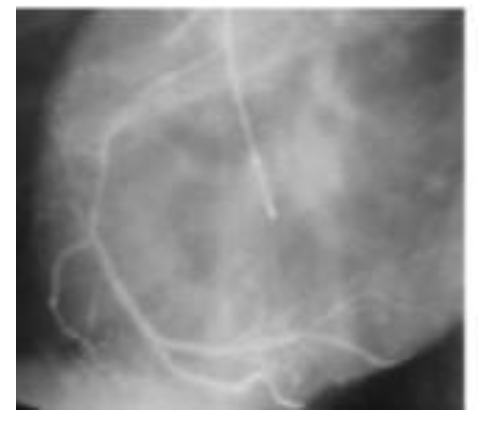
Before Dr. Rentrop’s arrival in the catheterization laboratory, the cardiologist performing the patient’s coronary angiography had found a small scar in the inferior wall, caused by the previous heart attack. The right coronary artery, which provides blood flow to the inferior wall, was severely narrowed in its middle segment (Figure 1). This is the original slide of that narrowing.
Three minutes after the second injection of contrast material into the right coronary artery the patient began to complain of chest pressure radiating into both arms which worsened rapidly. Only during his previous heart attack had he experienced symptoms of similar severity.
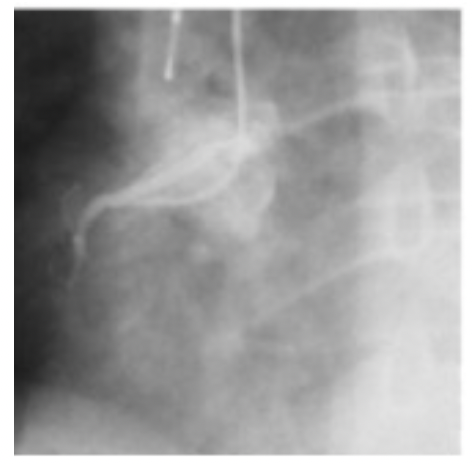
Since the changes in the electrocardiogram indicated that another heart attack was evolving in the distribution of the right coronary artery, Dr. K Peter Rentrop performed a third contrast injection into this vessel. It was now completely obstructed in the middle segment (figure 2).
What had happened?
Possible scenarios raced through Dr. Rentrop’s mind. A rare complication can occur when the catheter injures the vessel during coronary angiography, causing total occlusion. In this patient’s case, however, the angiogram did not show such damage. Another complication can happen if the catheter induces spasm of the vessel wall, which can also cause occlusion but can be resolved with nitroglycerin. For this patient, however, a 30-minute infusion of nitroglycerin did not improve his symptoms or electrocardiographic changes. The coronary occlusion persisted. His doctors now considered another rare complication of coronary angiography as the most likely cause of the abrupt obstruction. A blood clot had most likely formed on the surface of the catheter and washed down into the coronary artery, getting stuck in its severe narrowing. The patient was at the verge of losing the entire back wall and part of the side wall of his heart. Dr. Rentrop pondered how he could prevent this disastrous outcome. He found himself in more than one dilemma. He knew that the generally accepted treatment for heart attacks at the time, limited to bed rest, pain medication and treatment of irregular heartbeats, did not offer much hope for this patient. He also knew that the latest research about the cause and evolution of heart attacks contradicted the scientific principles underlying this standard treatment.
Pathologists debated the cause of heart attacks. One view, generally accepted by the 1930s, held that heart attacks result from occlusion of a coronary artery by a blood clot. The blood clot was thought to be triggered by rupture of a coronary blockage called plaque into the channel of the vessel. This view was challenged, however, in the late 1950s by some pathologists who found only severe chronic narrowing but no blood clots postmortem in the coronary arteries of most patients thought to have died from heart attacks. These pathologists proposed a second view. They suggested chronic plaques limited the blood flow and oxygen supply to the minimum necessary for the heart muscle to contract with normal force. In this line of reasoning, any decrease in blood flow which could be caused by a drop in blood pressure, or any increase in oxygen demand due to physical effort or stress, would result in insufficient oxygen supply to the heart muscle. Insufficient oxygen supply, they reasoned, is known to weaken the pump function of the heart and would set up a vicious circle of decreasing blood pressure and a further decrease of blood flow and oxygen supply, eventually culminating in death of heart muscle.
Pathologists continued to debate these two contradictory hypotheses for the next 20 years, but after the 1950s, clinical cardiologists embraced the second, demand/supply model. Therefore, standard treatment for heart attacks until the 1980s aimed at limiting damage to the heart muscle by minimizing oxygen requirements of the heart with bed rest for up to six weeks and administration of opiates to reduce pain related stress. Approximately 50 agents were tested to reduce oxygen demand or protect the heart muscle during a state of low oxygen supply. A skeptical British pathologist dubbed these medications “anti-infarct drugs”.
An alternative approach to limiting infarct size, based on the first pathological viewpoint, the clot/plaque rupture theory, was tested primarily outside of the United States in small trials. “Clot busters”, i.e. medications to dissolve blood clots, were infused to restore blood flow to the heart. In the United States, the FDA rejected this as a treatment option in 1977.
More and more convinced of his own understanding of the physiology supporting the two viewpoints, based on his clinical experience in research and clinical animal experiments, Dr. Rentrop had come to disagree with most of his clinical colleagues and believed that the clot/plaque rupture hypothesis was the correct one. He had been principal investigator of a research project which aimed at saving the lives of extremely ill heart attack patients whose circulation had collapsed due to cardiogenic shock. These patients had almost no chance of survival with the standard medical treatments of the time. However, a few research teams in the world, the Göttingen group among them, hoped that restoring blood flow by creating a detour around the blockage with emergency aortic coronary bypass surgery would improve the pump function of the heart sufficiently to save these patients’ lives.
Peter Rentrop had to perform high risk coronary angiograms to map out the surgical procedure for these patients. Thus, the Göttingen team was able to confirm reports from other centers that coronary angiography could be performed safely even in very sick patients, if their circulation was appropriately supported. Restoration of blood flow would eventually be the only treatment modality which could save patients with cardiogenic shock, although the death rate of patients in shock remains high to this day.
The angiograms in Dr. Rentrop’s shock patients showed that most infarct-related coronary arteries were completely blocked, not just severely narrowed, contradicting what clinical cardiologists believed at the time. Dr. Rentrop also noticed filling defects. He interpreted these to be clots. An internationally renowned cardiac pathologist at the University of Göttingen who staunchly defended the clot/plaque hypothesis, Professor D. Sinapius, examined the coronary arteries of the non-survivors in this shock study using more advanced, newer methods. In each case he showed Dr. Rentrop there was an occlusive thrombus overlying a ruptured plaque. The filling defects Dr. Rentrop had seen during catheterization on the angiograms corresponded exactly with blood clots postmortem. These observations supported their conviction that an occlusive thrombus caused heart attacks.
First percutaneous coronary intervention (PCI) during acute myocardial infarction:
Could the 45-year-old truck driver with his catheter-related blood clot be helped if blood flow could be restored to the occluded right coronary artery with aortocoronary artery bypass surgery? Perhaps. This was a definite option. An operating room would be available in about three hours. At the time, a three-hour delay was considered acceptable since it was believed that heart muscle starts dying only six hours after obstruction of a coronary artery.
However, a groundbreaking experimental study, published by Drs. Keith Reimer and Robert Jennings in October of 1976 showed that in dogs, heart muscle cells begin to die as soon as 20 minutes after occlusion of a coronary artery and that infarction is “complete” after 6 to 24 hours. Moreover, restoration of blood flow (called “reflow” or “reperfusion”) limited the extent of cell death depending on how long the heart muscle was deprived of oxygen-carrying blood flow. The benefit of reflow was greatest within 40 minutes after coronary occlusion but then continuously decreased over time. Could these findings in dogs be applicable to humans? If so, significant heart muscle damage would occur during the three hours wait for an operating room.
There was no definitive answer whether Reimer’s animal model also reflected the progression of heart muscle death in people after a coronary occlusion. However, Dr. Rentrop knew that the results of emergency bypass surgery performed in heart attack patients were consistent with Reimer’s findings in experimental animals. Poor outcomes were mostly reported among patients who presented late, more than 12 or even 24 hours after onset of infarction. Dr. Berg in Spokane, Washington, reported operating within 6 hours of infarct-onset, a timeframe he and his group developed based on their clinical observations. He reported hospital mortality rates of about 5%, which were so much lower than the death rate of 15% associated with medical therapy at the time, that the medical community largely disregarded them as not plausible.
As the patient’s symptoms and ominous ECG changes failed to improve during the nitroglycerin infusion, Dr. Rentrop concluded that rapid restoration of blood flow was the only possibility to avoid a major heart attack for this man. But how could this be achieved short of bypass surgery with its inherent delay?
The catheter, which had been used for contrast injection into the right coronary artery, was tantalizingly close to the obstruction. Could it be used as a tool for recanalization? Catheter-based techniques had been developed to reopen completely obstructed leg arteries by Dr. Charles Dotter, a radiologist who called the procedure “transluminal recanalization”. In this procedure, Dr. Dotter placed a catheter close to the obstruction of the leg artery and used a wire which he advanced through the catheter to perforate the obstruction. He enlarged the new channel by pushing a series of catheters of increasing diameter over the wire through the blockage.
Dr. Dotter’s equipment was not designed for intervention in the coronary arteries. Dr. Andreas Grüntzig’s balloon catheters, which had been introduced one year earlier to dilate chronic coronary artery narrowing but not acute total occlusion, were still being crafted for his personal use only.
When Dr. Rentrop reviewed his limited equipment, it occurred to him that the diameter of the flexible wires routinely used to guide catheters to the origin of the coronary arteries, roughly corresponded to the narrowed channel of the right coronary artery before the clot obstruction. Perhaps, he thought, sufficient blood flow could be restored by pushing the clot downstream into a small branch with a wire, where it would cause less damage to the patient than waiting for several hours. He had to weigh the possible risk that reflow might cause fatal irregularities of heart rhythm as it had in some of the dogs. In their experience with much sicker patients than this man, the Göttingen team knew they could safely stabilize life-threatening heart irregularities with new medications.
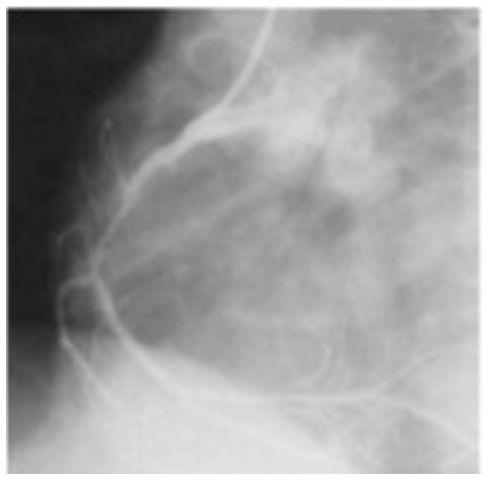
Dr. Rentrop decided to proceed. He maneuvered the catheter far into the right coronary artery close to the site of obstruction and advanced a guide wire of 0.8 mm diameter through the channel of the catheter to the obstruction. He then slid the wire across the obstruction. There was minimal resistance. He removed the guidewire and injected contrast media. The right coronary artery was open again! (Fig. 3)
Excited shouts came from the control room: “The electrocardiogram is normalizing!” The patient said his chest felt better. Within 8 minutes his symptoms had completely resolved. The heart attack had been stopped! The room was jubilant. No one had ever seen such a dramatic response to a heart attack by using medical treatment alone.
The patient was maintained on blood thinners to prevent re-occlusion of the vessel and remained stable until and through his bypass surgery three hours later. The surgeon noticed a small scar on the back wall of the heart from his previous heart attack 9 months earlier, but his heart contracted vigorously. Tests confirmed that only minimal new damage had occurred. The first percutaneous coronary intervention (PCI) to achieve reflow in a heart attack patient had stopped the progression of heart muscle death at its very start.
International recognition of primary percutaneous intervention (PCI) in stopping heart attacks:
The spectacular success of transluminal recanalization in removing a catheter-induced coronary thrombus inspired Dr. Rentrop to explore this technique in patients with spontaneous heart attacks caused by a thrombus due to plaque rupture. He developed guidewires to safely perforate coronary thrombi and tapered recanalization catheters to enlarge the channel. He tested them in dogs. In a proof-of-concept study he achieved recanalization in 9 of 15 patients with his technique. Heart muscle function improved following successful transluminal recanalization, whereas it deteriorated in a historical control group of patients in whom recanalization was not attempted.
Dr Rentrop presented the results of this pilot study to a standing ovation at the annual meeting of American Heart Association in Anaheim, California, in November of 1979. The angiograms, showing restoration of flow, the electrocardiograms exhibiting immediate resolution of infarct-related changes and the documentation of improved pump function of the heart convinced a large international audience of cardiologists that they had witnessed the beginning of a new era of infarct therapy.
Groups around the world immediately utilized his method and reproduced the results. Catheter-based reperfusion by transluminal recanalization initiated the era of “primary percutaneous coronary intervention” (PCI). Primary PCI was modified, and further developed by many investigators to its current level of effectiveness. A first step used Dr. Grüntzig’s balloon catheters to not only recanalize a total obstruction but to dilate the underlying plaque more efficiently. The potential of “balloon angioplasty,” became fully apparent after Dr. John Simpson developed a more steerable and safer balloon catheter/guidewire system. In 1983 Dr. Geoffrey Hartzler reported recanalization rates of 94% using this system. Ten years later, in 1993, a series of randomized trials reported superior clinical outcomes for heart attack patients treated with primary balloon angioplasty. Stents, developed in the late 1980s to improve long term outcomes in patients with chronic coronary artery disease, were eventually also used in primary PCI. Dr. Cindy Grines published a seminal trial in 1999, which showed that primary PCI with stents yields superior clinical results when compared with balloon angioplasty. In 2009, 30 years after its first use, United States and European guidelines finally recommended primary PCI as the preferred reperfusion strategy in acute heart attacks.
A recent analysis of the 2-year death rate among patients in rural hospitals in China highlights the clinical impact of primary PCI. In contrast to the US, modern heart attack treatments are not yet widely available in rural China. The 2-year death rate in rural China was 28.5% among patients who did not receive modern treatment, compared with 6.8% for those treated with primary PCI.
Since its inception during a catheterization accident 45 years ago, primary PCI has saved many millions of lives worldwide and continues to do so.







{kind=link}